A Patient's Guide to Osteoarthritis of the Elbow
Introduction
The elbow joint is injured less often than many other joints in the body. The most common injuries of the elbow joint are fractures and dislocations. Most elbow injuries tend to heal pretty well.
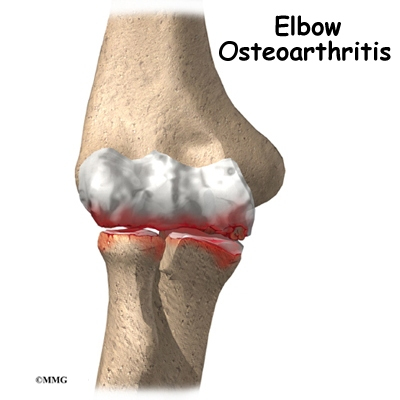
However, an elbow injury can lead to problems later in life. The injury changes the way the joint works just enough to cause extra wear and tear to the surfaces of the joint. Over time, the joint degenerates, causing pain and difficulty with daily activities. This condition is called osteoarthritis, degenerative arthritis, or posttraumatic arthritis.
This guide will help you understand
- how elbow osteorarthritis develops
- how elbow osteoarthritis is diagnosed
- what can be done to ease the pain and regain elbow movement
Anatomy
What parts of the elbow are affected?
The elbow joint is made up of three bones: the humerus bone of the upper arm, and the ulna and radius bones of the forearm.
The ulna and the humerus meet at the elbow and form a hinge. This hinge allows the arm to straighten and bend. The large triceps muscle in the back of the arm attaches to the point of the ulna (the olecranon). When the triceps muscle contracts, it straightens out the elbow. The biceps muscles in the front of the arm contract to bend the elbow.
View
animation of hinge movement
The connection of the radius to the humerus and the ulna allows the forearm to rotate. The upper end of the radius is round. It turns against the ulna and the humerus as the forearm and hand turn from palm down (pronation) to palm up (supination).
View
animation of elbow pronation/supination
In the elbow joint, the ends of the bones are covered with articular cartilage. Articular cartilage is a slick, smooth material. It protects the bone ends from friction when they rub together as the elbow moves. Articular cartilage is soft enough to act as a shock absorber. It is also tough enough to last a lifetime, if it is not injured.
Related Document: A Patient's Guide to Elbow Anatomy
Causes
What causes osteoarthritis?
Osteoarthritis is caused by degeneration of the articular cartilage of a joint. Degeneration is wear that happens over time. Doctors use the term degenerative arthritis to describe the wear and tear of a joint over many years. Degenerative arthritis is another term for osteoarthritis.
View
animation of degeneration
Some doctors use the term degenerative arthrosis. (Arthrosis just means that the joint is wearing out.) Arthritis is technically a condition of joint inflammation. Often, joints with osteoarthritis aren't inflamed. The term arthritis should really only be used to describe true inflammatory conditions, such as gout, infection, and rheumatoid arthritis.
A bad sprain or fracture can actually damage the articular cartilage. The cartilage can also be bruised when too much pressure is put on the cartilage surface. Osteoarthritis (OA) may be idiopathic, meaning there isn't a known reason for the condition. But most of the time, elbow osteoarthritis is linked with excess use of the arm.
The cartilage surface may not look any different. The injury often doesn't show up until months later. Sometimes the damage to the cartilage is severe. Pieces of the cartilage can actually be ripped away from the bone. These pieces do not grow back. Usually they must be surgically removed. If the pieces aren't removed, they may float around in the joint, causing it to catch. These pieces are referred to as loose bodies. They can also cause a lot of pain and do more damage to the joint surfaces.
Your body does not do a good job of repairing these holes in the cartilage surface. The holes fill up with scar tissue. Scar tissue is not as slick or rubbery as the articular cartilage.
An injury doesn't have to damage the cartilage to start the process of osteoarthritis. Any injury to the elbow joint can change the way the joint works. For example, after an elbow fracture the bone fragments may not line up exactly. They heal slightly differently from their condition before the injury. Even this slight difference can cause the joint to begin the cycle of wear and tear.
A dislocation can also cause lasting damage. After the ligaments have been injured in a dislocation, the elbow joint may move differently. This change in movement alters the forces on the articular cartilage. It's just like a machine, if the mechanism is out of balance, it wears out faster.
Over many years, this imbalance in joint mechanics can damage the articular cartilage. Since articular cartilage cannot heal itself very well, the damage adds up. Finally, the joint can no longer compensate for the damage, and the elbow begins to hurt.
Osteoarthritis of the elbow isn't like OA of the hip or knee. Most of the time, the articular cartilage isn't damaged. The joint space remains close to normal. The biggest changes are hypertrophic osteophyte (bone spur) formation and capsular contracture.
Capsular contracture refers to the process by which the capsule dries out and tightens up. The capsule has two layers: a fibrous covering that surrounds the joint and an inner lining. The inner layer is called the synovium. The synovial layer holds the lubricating fluid inside the joint.
Symptoms
What symptoms does osteoarthritis cause?
Pain and stiffness are the main symptoms of osteoarthritis of any joint. At first, the pain comes only with activity. Most of the time the pain lessens while doing the activity, but after resting for several minutes pain and stiffness increase. As the condition worsens, you may feel pain even when resting. The pain may interfere with sleep.
You may have swelling around your elbow. Your elbow joint may fill with fluid and feel tight, especially after using it. When all the articular cartilage is worn off the joint surface, you may begin hearing a squeak and feel a creak in the joint when you move your elbow. This creaking sensation is called crepitus.
Osteoarthritis eventually affects the elbow's motion. The elbow joint is one of the most sensitive to injury. It quickly becomes stiff and loses motion. The first thing most people notice is that it becomes hard to completely straighten the arm. Later they find it hard to bend.
Loss of motion leads to weakness and decreased function. Carrying heavy objects at the side of the body with the elbow straight is especially difficult.
Diagnosis
How will my doctor know if I have osteoarthritis?
The diagnosis of osteoarthritis of the elbow begins with a medical history of the problem. Your doctor will ask may questions about your pain, how it affects your daily activities, and any past injuries to your elbow. Because osteoarthritis develops over a long time, you may be asked questions about things you did long ago.
For example, throwing athletes (such as baseball pitchers) have a higher risk of developing osteoarthritis of the elbow later in life. Men with a history of heavy use of the arm are also at risk. This includes manual laborers and weight lifters.
Your doctor will also do a physical examination of the elbow and possibly other joints in the body. The moving and prodding may hurt, but it is important that your doctor sees exactly where and when you feel pain. Your doctor will feel for catching sensations as the joint moves. Catching may be caused by loose fragments of cartilage and bone. (These fragments are sometimes called joint mice.)
You will probably need to get standard X-rays. X-rays are usually the best way to see what is happening with your bones. X-rays can help your doctor assess the damage and track how your joint changes over time. X-rays can also help your doctor see how many bone spurs are present and if there are any loose bodies in the joint. X-rays also show the size of the joint space and how much articular cartilage is left.
CT scans give a 3-D view to show the size and location of any bone spurs present. CT scans can reveal osteophytes that don't appear on plain X-rays. CT scans also show the surgeon how close the bone spurs are to the ulnar nerve. This information is very useful when planning surgery to remove the spurs.
Your doctor may order blood tests if there is any question about the cause of your osteoarthritis. Blood tests can show certain systemic diseases, such as rheumatoid arthritis.
Treatment
What can be done to get rid of my pain?
Nonsurgical Treatment
In almost all cases, doctors try nonsurgical treatments first. Surgery is usually not considered until it has become impossible to control your symptoms.
The goal of nonsurgical treatment is to help you manage your pain and use your elbow without causing more harm. Your doctor may recommend nonsteroidal anti-inflammatory drugs (NSAIDs), such as aspirin and ibuprofen, to help control swelling and pain. Other treatments, such as heat, may also be used to control your pain.
Rehabilitation services, such as physical and occupational therapy, have a critical role in the treatment plan for elbow osteoarthritis. The main goal of therapy is to help you learn how to control symptoms and maximize the health of your elbow. You'll learn ways to calm your pain and symptoms. You may use rest, heat, or topical rubs.
You may be issued a special elbow splint to immobilize and protect the elbow. Resting the joint can help ease pain and inflammation. Range-of-motion and stretching exercises can improve your elbow flexibility. Strengthening exercises for the arm help steady the elbow and protect the joint from shock and stress. Your therapist will give you tips on how to get your tasks done with less strain on the joint.
To get rid of your pain, you may also need to modify or limit your activities. You may even need to change jobs, if your work requires heavy, repetitive motions with the hand and wrist.
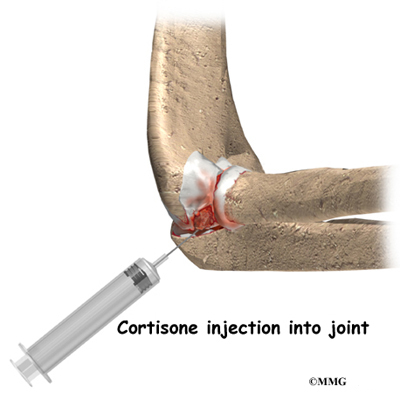
An injection of cortisone into the elbow joint can give temporary relief. Cortisone is a powerful anti-inflammatory medication. It can very effectively relieve pain and swelling. Its effects are temporary, usually lasting several weeks to months. There is a small risk of infection with any injection into the joint, and cortisone injections are no exception.
Surgery
Eventually, it may be necessary to consider some type of surgical treatment. There are several operations to treat advanced osteoarthritis of the elbow. Your surgeon will consider many factors when deciding which procedure is best for you, including the severity of joint degeneration, your age, your activity level, and how you use your elbow.
Arthroscopic Debridement
If you are in an early stage of osteoarthritis, your doctor may recommend arthroscopic debridement. Other names for this procedure include arthroscopic ulnohumeral arthroplasty or osteocapsular arthroplasty.
Arthroscopic procedures use an arthroscope, a tiny TV camera that is inserted into the joint through a very small incision. The arthroscope allows the surgeon to see inside the elbow joint.
In arthroscopic debridement, the surgeon makes other small incisions for inserting special tools to get rid of bone spurs, remove loose bodies, or smooth the cartilage. Sometimes a capsular release is needed. The capsule is a fibrous covering around the joint. An incision is made in the tissue and the anterior (front) of the capsule is removed.
Your surgeon may also do lavage in the joint. Lavage involves rinsing the joint with a sterile saltwater solution. Lavage helps remove tiny debris that may be irritating the joint. The arthroscope allows the surgeon to watch what he or she is doing on a TV screen during the procedure.
The majority of patients treated with arthroscopic debridement for elbow osteoarthritis have less pain and more motion after surgery. Symptoms may come back in some patients, but they are usually less severe.
Interposition Arthroplasty
Before the invention of high-quality artificial joints, surgeons used many techniques to keep the bone surfaces of arthritic joints from rubbing against each other. One of these techniques is distraction interposition arthroplasty. This procedure involves placing a piece of tendon or fascia between the bony surface of the elbow joint. (Fascia is a connective tissue, similar to tendon, that lies in a flat sheet. It covers the muscles and acts as a divider between different compartments of the body.)
As the joint heals, the tendon or fascia forms a cushion of thick, tough tissue between the bones. The tissue pads the ends of the bones and reduces pain while still allowing the elbow to move.
Interposition arthroplasty is rarely indicated but may be used in rare cases. It works fairly well in the elbow. It doesn't work very well in the weight-bearing joints of the hip, knee, and ankle.
Related Document: A Patient's Guide to Interposition Arthroplasty of the Elbow
Elbow Fusion
A fusion surgery (also called arthrodesis) eliminates pain by making the bones of the joint grow together, or fuse, into one solid bone. Fusions were very common before the invention of artificial joints. Even today, joint fusions are commonly used in many different joints to get rid of the pain of arthritis.
An elbow fusion will greatly decrease the motion in your arm. However, it does leave you with a strong and pain-free elbow. People who need a good range of motion in their elbow should consider another type of operation, such as an elbow joint replacement.
Related Document: A Patient's Guide to Elbow Fusion
Elbow Joint Replacement
Elbow joint replacement or total elbow arthroplasty (TEA) is not nearly as common as hip, knee, or shoulder replacement. This is true for a couple of reasons. Osteoarthritis in the elbow is not as common as osteoarthritis in weight-bearing joints.
Elbow joint replacement also has a higher complication rate than the more common replacement surgeries. Infection and slowed healing in the surgical incision are two complications of this type of procedure. Fracture, dislocation, and loosening are other problems reported with total elbow arthroplasty (TEA).
The elbow joint replacement is a good choice for patients who need improved motion rather than strength. Older patients who don't need as much strength will probably prefer the results of elbow replacement surgery. They must be willing to accept low levels of activity involving the elbow. Patients with advanced rheumatoid arthritis are also good candidates for total elbow arthroplasty (TEA).
Related Document: A Patient's Guide to Artificial Joint Replacement of the Elbow
Rehabilitation
When will I be able to use my elbow again?
Nonsurgical Rehabilitation
If you don't need surgery, range-of-motion exercises for the elbow should be started as pain eases. These exercises are followed by a program of strengthening that may include shoulder and upper back exercises. You'll be given tips on keeping your symptoms under control. You will probably progress to a home program within four to six weeks.
After Surgery
Your elbow will be bandaged with a well-padded dressing and an elbow splint for support. Physical or occupational therapy sessions may be needed for up to three months after surgery. The first few treatment sessions will focus on controlling the pain and swelling from surgery. You will then begin to do exercises that help strengthen and stabilize the muscles around the elbow joint. Your therapist will give you tips on ways to do your activities without straining your elbow.
|





