What can be done for the condition?
Nonsurgical Treatment
OA can't be cured, but therapies are available to ease symptoms and to slow down the degeneration. Recent information shows that mild cases of knee OA may be maintained and in some cases improved without surgery.
Medication
Your physician may prescribe medicine to help control your pain. Acetaminophen (Tylenol®) is a mild pain reliever with few side effects. Some people may also get relief of pain with anti-inflammatory medication, such as ibuprofen and aspirin. Newer anti-inflammatory medicines called COX-2 inhibitors show promising results and don't cause as much stomach upset and other intestinal problems.
Related Document: A Patient's Guide to Medications for Arthritis
Medical studies have shown that glucosamine and chondroitin sulfate can also help people with knee OA. These supplements seem to have nearly the same benefits as anti-inflammatory medicine with fewer side affects. Many doctors feel the research supports these supplements and are encouraging their patients to use them.
Related Document: A Patient's Guide to Glucosamine and Chondroitin Sulfate for Knee Osteoarthritis
If you aren't able to get your symptoms under control, a cortisone injection may be prescribed. Cortisone is a powerful anti-inflammatory medication, but it has secondary effects that limit its usefulness in the treatment of OA. Multiple injections of cortisone may actually speed up the process of degeneration.
Repeated injections also increase the risk of developing a knee joint infection, called septic arthritis. Any time a joint is entered with a needle, there is the possibility of an infection. Most physicians use cortisone sparingly, and avoid multiple injections unless the joint is already in the end stages of degeneration, and the next step is an artificial knee replacement.
A new type of injectable medication has become available in the United States. Hyaluronic acid has been used in Europe and Canada for several years. Doctors inject three to five doses into the joint over a one-month period. The medicine helps lubricate the joint, ease pain, and improve people's ability to get back to some of the activities they enjoy. Some people have had good results for up to eight months after getting these treatments.
Related Document: A Patient's Guide to Viscosupplementation for Knee Osteoarthritis
Physical Therapy
Physical therapy plays a critical role in the nonoperative treatment of knee OA. A primary goal is to help you learn how to control symptoms and maximize the health of your knee. You will learn ways to calm pain and symptoms, which might include the use of rest, heat, or topical rubs.
Physical therapists teach their patients how to protect the arthritic knee joint. This starts with tips on choosing activities that minimize impact and twisting forces on the knee. People who modify their activities can actually slow down the effects of knee OA. For instance, people who normally jog might decide to walk, bike, or swim to reduce impact on their knee joint. Sports that require jumping and quick starts and stops may need to be altered or discontinued to protect the knee joint.
Shock-absorbing insoles placed in your shoes can also reduce impact and protect the joint. In advanced cases of knee OA or when the knee is especially painful, a cane or walker may be recommended to ease joint pressure when walking. People who walk regularly are encouraged to choose a soft walking surface, such as a cinder or grass track.
A new type of knee brace, called a knee unloading brace, can help when OA is affecting one side of the knee joint. For example, a bowlegged posture changes the way the knee joint lines up. The inside (medial) part of the knee joint gets pressed together. The cartilage suffers more damage, and greater pain and problems occur. The unloading brace pushes against the outer (lateral) surface of the knee, causing the medial side of the joint to open up. In this way, the brace shares the pressure and unloads the arthritic medial side of the joint. A knee unloading brace can help relieve pain and allow people to do more of their usual activities.
For mild cases of knee OA, you may be given a heel wedge to wear in your shoe. By tilting the heel, the wedge alters the way the knee lines up, which works like the unloading brace mentioned above to take pressure off the arthritic part of the knee.
Range-of-motion and stretching exercises will be used to improve knee motion. You will be shown strengthening exercises for the hip and knee to help steady the knee and give additional joint protection from shock and stress. People with knee OA who have strong leg muscles have fewer symptoms and prolong the life of their knee joint. Your therapist will also suggest tips for getting your tasks done with less strain on the joint.
Surgery
In some cases, surgical treatment of OA may be appropriate.
In cases of advanced OA where surgery is called for, patients may also see a physical therapist before surgery to discuss exercises that will be used just after surgery and to begin practicing using crutches or a walker.
Arthroscopy
Surgeons can use an arthroscope (mentioned earlier) to check the condition of the articular cartilage. They can also clean the joint by removing loose fragments of cartilage. People have reported relief when doctors simply flush the joint with saline solution. A burring tool may be used to roughen spots on the cartilage that are badly worn. This promotes growth of new cartilage called fibrocartilage, which is like scar tissue. This procedure is often helpful for temporary relief of symptoms for up to two years.
Related Document: A Patient's Guide to Arthroscopy
Proximal Tibial Osteotomy
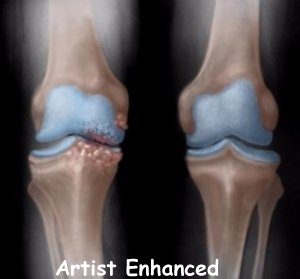
OA usually affects the side of the knee closest to the other knee (called the medial compartment) more often than the outside part (the lateral compartment). OA in the medial compartment can lead to bowing of the knee. As mentioned earlier, a bowlegged posture places more pressure than normal on the medial compartment. The added pressure leads to more pain and faster degeneration where the cartilage is being squeezed together.
Surgery to realign the angles in the lower leg can help shift pressure to the other, healthier side of the knee. The goal is to reduce the pain and delay further degeneration of the medial compartment.
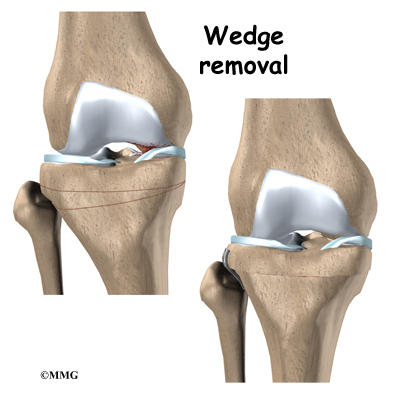
One procedure to realign the angles of the lower leg is called a proximal tibial osteotomy. In this procedure, the upper (proximal) part of the shinbone (tibia) is cut, and the angle of the joint is changed. This converts the extremity from being bowlegged to straight or slightly knock-kneed. By correcting the joint deformity, pressure is taken off the cartilage. A proper joint angle actually allows the cartilage to regrow, a process called regeneration.
This surgical procedure is not always successful. Generally, it will reduce your pain but not eliminate it altogether. The advantage to this approach is that very active people still have their own knee joint, and once the bone heals there are no restrictions on activities.
A proximal tibial osteotomy in the best of circumstances is probably only temporary. It is thought that this operation buys some time before a total knee replacement becomes necessary. The benefits of the operation usually last for five to seven years if successful.
Related Document: A Patient's Guide to Tibial Osteotomy
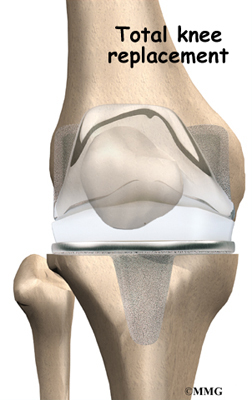
Artificial Knee Replacement
An artificial knee replacement is the ultimate solution for advanced knee OA.
Surgeons prefer not to put a new knee joint in patients younger than 60. This is because younger patients are generally more active and might put too much stress on the joint, causing it to loosen or even crack. A revision surgery to replace a damaged prosthesis is harder to do, has more possible complications, and is usually less successful than a first-time joint replacement surgery.
Related Document: A Patient's Guide to Artificial Joint Replacement of the Knee
What should I expect after treatment?
Nonsurgical Rehabilitation
Nonsurgical treatments are used to maximize the health of your knee and to prolong the time before surgery is needed. Physical therapy may be needed to ease pain and improve mobility, strength, and function. The focus of these visits is to help you learn to control symptoms as well as learn strategies to protect your knee over the years. You will probably progress to a home program within two to four weeks.
After Surgery
Physical therapy treatments after surgery depend on the type of surgery performed. Rehabilitation is generally slower and more cautious after knee replacement procedures and certain types of tibial osteotomies. After simple procedures such as arthroscopy, you may begin fairly aggressive exercise therapy immediately.
Therapy treatments usually begin the next day after surgery. Your first few rehabilitation sessions are used to ease pain and swelling, help you begin gentle knee motion and thigh tightening exercises, and get you up and walking safely. You may need to use either a walker or crutches after surgery. Some patients may be instructed to limit how much weight they place on the knee for four to six weeks.
After going home from the hospital, some patients may be seen for a short period of home therapy before beginning outpatient physical therapy. Outpatient treatments are designed to improve knee range of motion and strength and to safely progress your ability to walk and do daily activities.
The therapist's goal is to help you keep your pain under control, maximize knee mobility, and improve muscle strength and control. When you are well under way, regular visits to your therapist's office will end. The therapist will continue to be a resource, but you will be in charge of doing your exercises as part of an ongoing home program.