A Patient's Guide to Spinal Tumors
Introduction
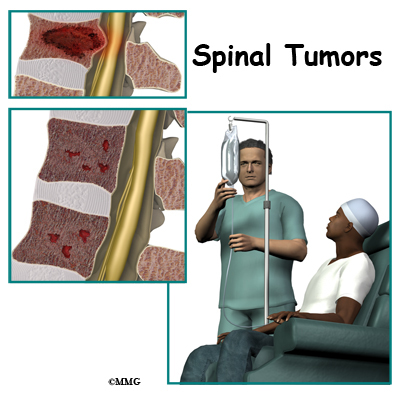
A tumor is an abnormal growth of tissue. There are several types of tumors that can develop in or near the spine. There are many types of spinal tumors. They can involve the spinal cord, nerve roots, and/or the vertebrae (bones of the spine) and pelvis.
There are two classifications of spine tumors. A spinal tumor can be primary, meaning it comes from cells within or near the spine. Primary tumors of the spine are rare. More commonly a spinal tumor that is found is a secondary spinal tumor. This means that the tumor traveled there from somewhere else in the body.
Tumors can be benign (non-cancerous) or malignant (cancerous).
This guide will give you a general overview of spinal tumors and help you understand
- what parts of the spine are involved
- what causes spinal tumors
- how doctors diagnose the condition
- what treatment options are available
Anatomy
What parts of the spine are involved?
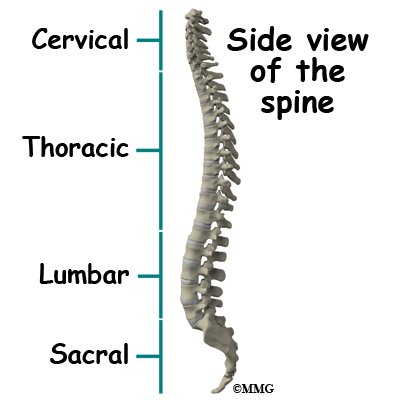
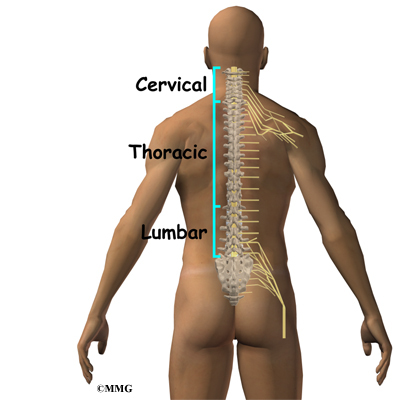
The cervical spine is formed by the first seven vertebrae. The cervical spine starts at the bottom edge of the skull. It ends where it joins the top of the thoracic spine. The thoracic spine is where the chest begins and is made up of twelve vertebrae. This region is different than the other areas of the spine because it has ribs attached to the vertebrae. It ends where it joins with the lumbar spine. The lumbar spine is made up of five vertebrae in the lower back. It joins with the sacrum or pelvis at the bottom.
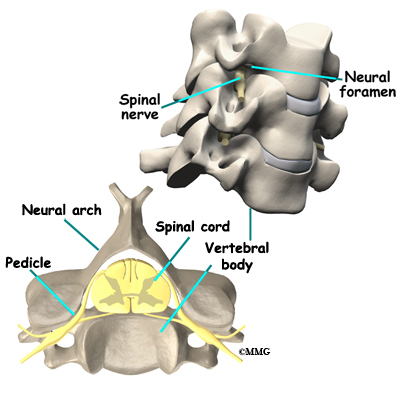
Each vertebra is formed by a round block of bone, called a vertebral body. A bony ring attaches to the back of the vertebral body. When they are stacked on top of one another, the rings form a hollow tube called a neural arch. This forms a canal where the spinal cord is located. The spinal cord is protected by the bone. The spinal cord begins at the base of the brain, just below the medulla or brain stem. It ends in the lumbar spine at about the first or second lumbar vertebrae where it is called the conus medullaris. Here it splits into many fibers. This is called the cauda equina because it looks like a horse's tail.
The spinal cord is a tube of nerve cells that is hollow in the middle. It carries sensory and motor messages to and from the body and the brain. It is surrounded by layers of tissue and fluid called the cerebral spinal fluid. It is housed in the vertebral or spinal column which is made up of 24 bones, called vertebrae. Vertebrae are stacked on top on one another to form the spinal column. The spinal column is the body's main upright support.
There are three layers of tissue that surround the spinal cord. The thin, delicate lining of the spinal cord is the pia mater. The next layer is the arachnoid membrane. It was named that because it looks like a spider web. The outermost layer that is thicker and tougher is called the dura mater. These layers are continuous with the layers covering the brain. These layers may give rise to tumors that can spread to the spinal cord.
Related Document: A Patient's Guide to Lumbar Spine Anatomy
Causes
What causes this problem?
A primary spinal tumor means it comes from cells within or near the spine. They can involve the spinal cord, nerve roots, and/or the vertebrae (bones of the spine) and pelvis.They can be benign (non-cancerous) or malignant (cancerous). In general, benign tumors do not invade other tissues. Malignant tumors may invade other tissues and organs in the body. Although primary spinal tumors often contain a number of abnormal genes their cause remains unknown. In some cases the tumors run in families.
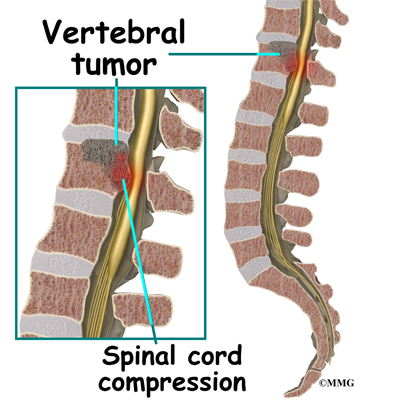
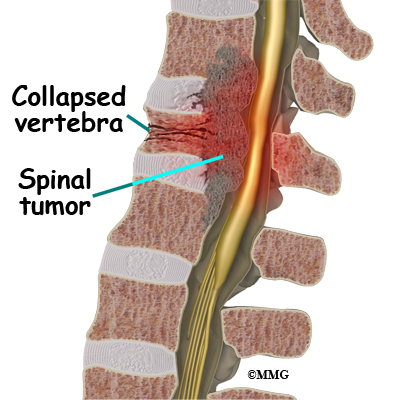
Tumors in the spine become a problem when they compress the spinal cord or nerves. This can lead to serious complications such as paralysis and loss of bladder and bowel control. Others can destroy the vertebral bone that supports the spinal cord making it unstable.
Nerve roots on either side of each spinal segment are made up of bundles of motor and sensory nerves that come from the spinal cord. Nerves are covered by protective cells called Scwhann cells. A form of spinal tumor involving the Schwann cells is called a Schwannoma.
A secondary spinal tumor is more common. This means that the tumor traveled there from cancer somewhere else in the body. These secondary or metastasized tumors are always cancerous. These cancer cells travel and cause tumors that usually involve the vertebrae or bony portion of the spine. They may come from melanoma (skin cancer), cancer in the lung, breast, prostate, kidney, or thyroid gland for example.
Symptoms
What does a spinal tumor feel like?
Sometimes the tumors are found before they cause any symptoms. The symptoms will vary depending on where the tumor is located and what tissues are involved.
At times, pain, bowel or bladder problems, sexual dysfunction, change in sensation, or muscle weakness of the arms or legs may alert you to the problem. This often means that the tumor is compressing the spinal cord or nerve root. Tumors that originate in the spinal cord itself may not cause pain. Pain that awakens you in the night or development of scoliosis (abnormal spine curve) may be a sign that the bone of the vertebra is being destroyed by a spinal tumor.
Symptoms may have a gradual or rapid onset. Symptoms usually worsen without treatment.
Diagnosis
How will my doctor diagnose the problem?
Diagnosis begins with a thorough history and physical exam. Your doctor will ask questions about your symptoms and how your problem is affecting your daily activities. This will include questions about pain, feelings of numbness or weakness, change in bowel or bladder function, and whether you have noticed any changes in the way you walk. Your doctor will want to know if have been diagnosed with any type of cancer in the past.
During the physical exam, sensation of the skin, muscle strength, and reflexes are tested. Your doctor may ask you to walk to see if there are any changes in your walking pattern.
In addition to having lab work done, there are several procedures that can help your doctor diagnose a spinal tumor.
Magnetic resonance imaging (MRI) allows your doctor to look at slices of the area in question. The MRI machine uses magnetic waves, not X-rays to show the soft tissues of the body. This includes the spinal cord and nerves. The test may require the use of dye that is given intravenously.
Computed tomography (CT) scan may be ordered when an MRI is unavailable. Dye will be introduced into the spinal canal fluid so that the spinal cord and nerve root anatomy are identified better. When dye is injected for this purpose, the technique is called a myelogram.
X-rays of the spine may be ordered when there is the likelihood of metastasized tumor from cancer elsewhere. It can show only changes in the bones. Many primary spinal tumors do not affect the bone when they are in the early stage.
Bone scans can be used to detect fracture, bone infection, or cancer. A radioactive tracer, technetium (Tc), is injected into your vein. Where there is an increase in metabolic activity, such as is the case with cancer, the Tc will be more concentrated. Spinal tumors may be malignant, or metastasized from cancer somewhere else in the body. It is helpful to use a scan to see if there are other areas in the body where the cancer may be.
A biopsy helps determine the type of the tumor. A biopsy may require surgery. Sometimes it can be performed using a needle while using CT for guidance. A piece of the tumor is removed and looked at under a microscope.
Types of Spinal Tumors
Malignant Spinal Tumors
Osteosarcoma occurs most often in children, adolescents, and young adults. Males are more likely to be affected than females. Treatment usually consists of removal of the tumor when possible as well as chemotherapy. Radiation therapy is not effective. Older persons with Paget's disease or who have had radiation therapy may develop this type of tumor.
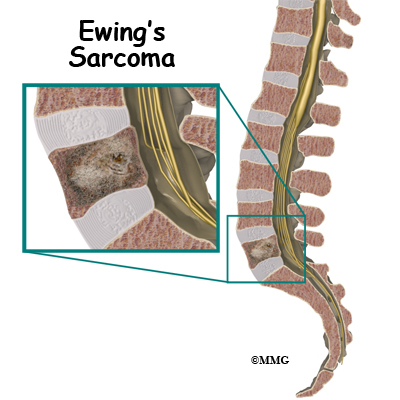
Ewing's Sarcoma occurs in the bone of the spine or surrounding tissues. It usually affects adolescents and those in early adulthood. When it involves the spine, it may cause paralysis and loss of bladder or bowel function (incontinence), numbness or tingling. Removing the tumor is preferred if possible, in combination with chemotherapy and sometimes radiation. If the tumor has traveled to the bone marrow, stem cell transplant is a more aggressive form of treatment.
Chondrosarcoma usually occurs in adults and is most common in flat bones such as the pelvis. They usually are noticed because they cause pain and swelling. Surgery is performed to remove the tumor and any tumors that have spread, usually to the lung. In most cases, chemotherapy is not effective.
Astrocytomas are tumors that involve nerve cells within the spinal cord and brain. They most commonly occur in children and adolescents. Neurological symptoms such as weakness and/or sensory changes may be the cause for seeking treatment. They tend to spread throughout the spinal cord and brain. Astrocytomas in the spine can usually be removed surgically. However, they are difficult to completely remove. Radiation therapy may be necessary following surgery to slow the spread of the tumor.
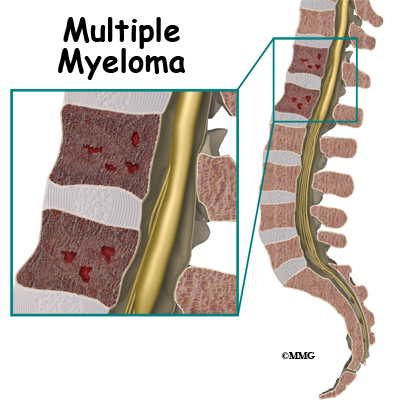
Cancer in the bone marrow is called multiple myeloma. Bone tissue is destroyed by excessive growth of plasma cells in the bone marrow. When X-rayed it appears that holes have been taken out of the bone. These are called osteolytic lesions. Plasma cells are part of the immune system and in multiple myeloma they grow uncontrolled forming tumors in the bone marrow. Any part of the skeletal system (bones) can be affected including the spine. For multiple myeloma, treatment may include chemotherapy and other medications, radiation, and stem cell transplantation.
Benign Spinal Tumors
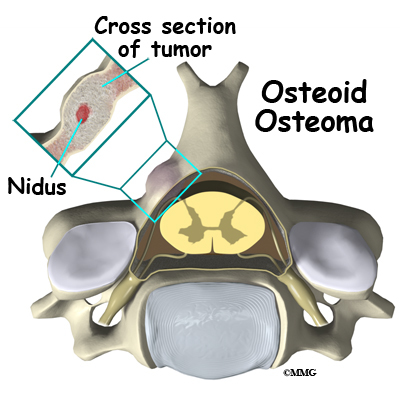
Osteoid osteoma is the most common of the benign tumors involving the bone of the spine. It is usually found during adolescence. It may be discovered because of scoliosis or curvature of the spine. It may cause pain that does not ease up, and is worse at night. Anti-inflammatory medications are used for treatment. Sometimes removal of the tumor by surgery is necessary. A newer, less invasive treatment is called radio-frequency ablation. These tumors rarely recur (come back).
Related Document: [relateddocument id=""]A Patient's Guide to Pain Management: Radiofrequency Ablation[/relateddocument]
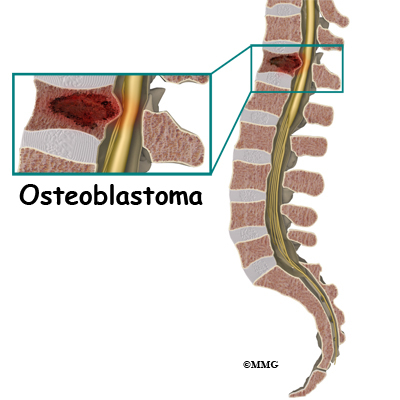
Osteoblastomas are larger versions of osteoid osteomas. They tend to be found in people under the age of 30. They may cause scoliosis or curvature of the spine. Osteoblastomas tend to be more aggressive and require surgery to remove the tumor. There is a 10% chance that the tumor may recur.
Giant cell tumors are very rare and tend to affect the vertebral body of a spinal segment. They can be aggressive and sometimes spread to other parts of the body, usually the lung. Treatment involves surgery to remove the tumor. Also, radiation therapy may be used.
Enchondromas are tumors involving cartilage. They may grow into the spinal canal or press on the spinal nerve roots. When they cause paralysis, bowel or bladder incontinence, or other neurological symptoms they are surgically removed. They rarely can become chondrosarcomas, which are malignant tumors that can spread to other parts of the body.
Hemangiomas are tumors involving blood vessels that affect the vertebral body of a spinal segment. They are most commonly found in the thoracic or lumbar portion of the spine. They occur more frequently during mid-life. They are found more often in women than men. They can be a source of pain but often do not cause pain. They may be large enough to cause collapse of the vertebral body which could affect the spinal cord or nerve roots.
Meningioma is the most common spinal cord tumor. They tend to occur in older adults and are more common in women. They are usually treated with surgical removal. Rarely, meningiomas recur or spread to other parts of the body.
Ependymoma is a tumor involving the cells lining the canal in the center of the spinal cord. These tumors have the greatest chance for surgical cure.
Schwannoma is a tumor that involves the covering or sheath of peripheral nerve fibers. It may cause weakness, paralysis or sensory changes such as numbness. It can be removed surgically.
Chordomas are tumors that are typically found at the lower end of the spine. Because they can aggressively grow, they can cause compression of the spinal cord or nerve roots causing neurological problems. Treatment involves surgery to remove the tumor. Unfortunately they come back, but do not spread to other areas of the body.
Plasmacytoma is a single tumor involving the bone of a spinal segment. It can have characteristic punched out holes in the bone on X-ray. It can cause a compression fracture of the vertebral body. This can cause neurological symptoms. Spinal surgery to decrease pain and improve function may be necessary. Plasmacytoma is felt to be an isolated form of multiple myeloma, which will then develop lesions in other bones in the body. Multiple myeloma is a malignant process and is the most common primary bone cancer.
Treatment
What treatment options are available?
The type of treatment will depend on symptoms, general health, the results of imaging studies, and a biopsy if done. Many times a combination of surgical and non-surgical treatments are required. If your treatment involves radiation or chemotherapy, you will be asked to see an oncologist (a doctor that specializes in cancer).
Early diagnosis and treatment of a spinal tumor is important. If undiagnosed, the damage caused by the tumor can become permanent.
Nonsurgical Treatment
Sometimes watching the tumor for growth is all that is necessary if significant symptoms are not present. The tumor is monitored with repeat imaging such as MRI. Not all spinal tumors can be removed by surgery due to their location.
A back brace or corset may help to stabilize the spine. This should also reduce pain. It may need to be custom made to fit you.
Medications such as corticosteroids may be prescribed. They are used to decrease the swelling in the spinal cord that can cause compression. They may be taken temporarily or long-term to relieve symptoms. Analgesics such as narcotics may also be used. Medications that diminish the blood supply to the tumor have shown some success. Bisphosphonates are medications more commonly used for osteoporosis. They may be used to treat tumors that can destroy bone in the spine.
Embolization is a term used when the blood supply to a tumor is interrupted. This is done by burning the blood vessel(s). Several types of spinal tumors are treated using this method.
Chemotherapy is used if the primary tumor is a malignant or cancerous tumor. Chemotherapy is also recommended when the tumor is a secondary tumor that has traveled from another area in the body and invaded spinal tissue.
Radiation therapy may also be used to treat tumors that cannot be removed by surgery.
Stem cell transplant may be used for aggressive cancers such as Ewing's sarcoma.
Surgery
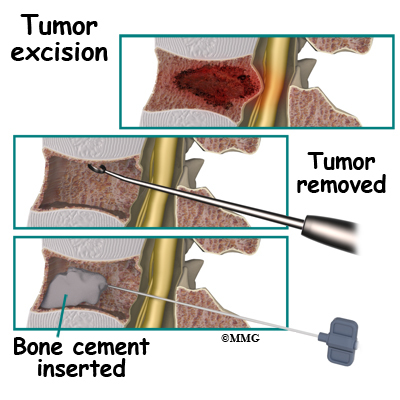
Surgery may be the only treatment for a primary spinal tumor that is non-cancerous. As much of the tumor is removed as possible without causing neurological problems. A decompression refers to removing bone around the spinal cord or spinal nerves in order to take pressure off these structures. Neurological damage during surgery has been improved with the use of newer techniques. These techniques include ultrasonic aspirators, and microsurgery. Ultrasonic aspirators use sound waves to destroy the tumor. It also sucks up the pieces of tumor. Microsurgery uses a microscope for a better view of the operation site. This helps to minimize any damage to surrounding healthy tissue.
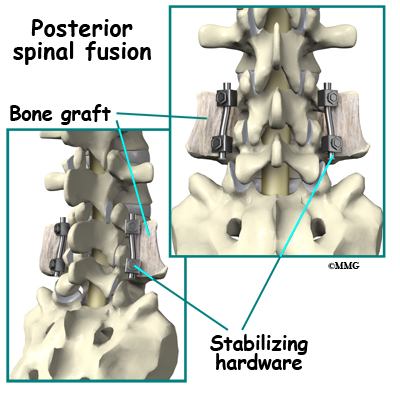
If the spine needs to be stabilized or fused as a result of removing a tumor in bone, metal hardware may be required. Metal plates, cages, rods, or screws may be used. The bone may be additionally supported by bone graft or bone cement.
Rehabilitation
What should I expect after treatment?
Nonsurgical Rehabilitation
Your doctor will require you to have periodic follow-up. New lab tests and imaging studies may be required. You may need pain management on a regular basis.
Physical therapy can help with balance, strength, walking, and coordination. Occupational therapy helps with activities of daily living such as dressing, bathing and assistance with mobility. You may need instruction in the use of a brace. Instruction in proper ways to lift and move may be necessary.
After Surgery
The amount of time you will be hospitalized depends on the type of surgery required.
After surgery, activity such as sitting and walking will be allowed as well as activities that do not require stretching of the spine or straining. Lifting is limited during the initial recovery period. You may be required to use a brace or corset after surgery to help with stability.
Radiation is often used following surgery to kill remaining tumor cells. It usually begins one to two weeks following surgery. Radiation lasts only 15-20 minutes per day for two to six weeks.
You can expect recovery and improvement in symptoms between two weeks and several months following surgery. You may need pain management during your recovery, or possibly on a more long-term basis.
Physical and occupational therapy may be beneficial to help restore any lost strength, coordination, or other skills.
Your surgeon will require you to have periodic follow-up. New lab tests and imaging studies may be required. Sometimes the tumor will grow back and need to be removed again.
|





